
In a previous blog, Salivary Diagnostics—Your Molecular X-ray,
I introduced the concept of using salivary diagnostics to provide objective understanding to the clinical signs observed with periodontal disease. Once a saliva specimen is analyzed and the results released, the clinician must correlate the lab results to the clinical signs, and decide the next steps for treatment. One feature of the MyPerioPath® test report is the “Reference Lines,” displayed as black lines overlying the bars which represent the measure of each bacteria assayed. This blog will provide the origins of those Reference Lines, and how clinicians should consider the results of each patient, relative to those levels. It will also explain the role these Reference Lines play with systemic antibiotic suggestions and review an alternative option to Reference Lines for consideration.
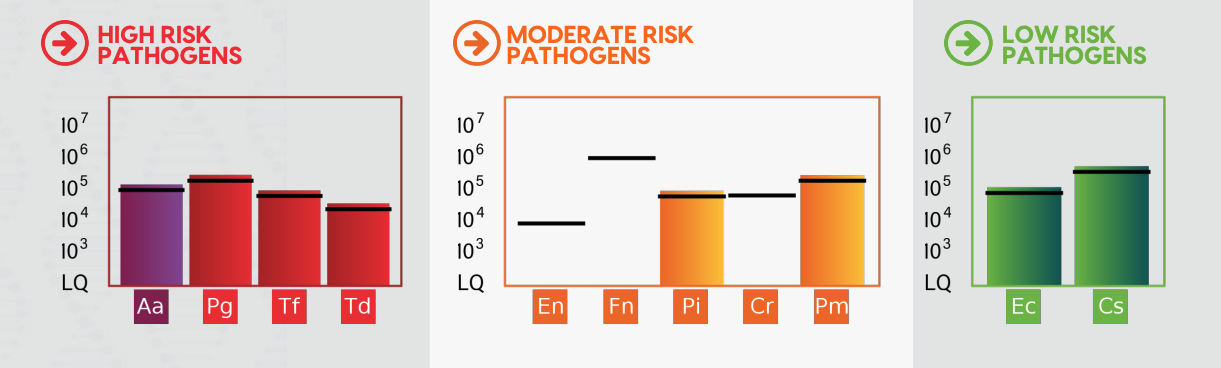
The Basis of the Reference Lines: The Reference Lines help the clinician align/confirm their assessment of the severity of the clinical signs (BOP, pocket depth, radiographic evidence of bone loss, attachment loss) with the quantity of bacteria typically measured with those clinical features. The definition of the MyPerioPath reference lines takes into consideration patient results representing varying backgrounds/situations and it is the mean quantity of each of the 11 bacteria present in patients with (clinically observable) chronic periodontitis. The Reference Lines represent a midpoint of the amount of bacteria correlated with a certain severity of clinical disease. The statistical power of these analyses is extraordinary and reliable.
Other Risk Factors and the Patient’s Personal Tipping Point: Deciding who and how to treat is ultimately based on clinical findings and determined by the treating healthcare professional. The Reference Lines displayed on each result report should be a guidepost to ask “What other parts of this patient’s health might raise or lower the black lines, reflecting their personal tipping point?” Diabetes is one obvious systemic risk factor that is likely to decrease the patient’s personal tipping point. Smoking is another. In both cases there is the altering of the person’s immune function that gives rise to the clinical signs of inflammation and chronic effects of tissue damage with lesser levels of these key pathogens. Genetic susceptibility manifests greater than needed levels of chronic inflammation, also possibly lowering the patient’s personal tipping point. There are several genetic salivary tests for the clinician to consider for objective and concrete information regarding a patient’s genetic risk, such as MyPerioID® IL-6 (part of Alert 2™) and Celsus One™. This is a limited list of other risk factors that may impact the patient’s personal tipping point. For this reason, a complete review of the medical history with each patient is always the standard of care, and critical to uncover other important risk factors.
The Systemic Antibiotic Selection: The Reference Lines are not the basis by which a clinician should choose to use an antibiotic. Rather, the black lines on each MyPerioPath® report serve as an indicator of a consensus regimen for the selection of which antibiotic to prescribe. When there is a single bacteria, or combination of bacteria, above the reference line, an antibiotic(s) selection will be inserted in the Treatment Suggestions section of the report (if you select to have the option displayed upon ordering). If the bacteria are present but below the reference line, a resource called MyPerioPath® Antibiotic Options, is available for the clinician to determine the most appropriate antibiotic option(s).
Alternative to Reference Lines: Some clinicians prefer to base treatment options on total bacterial load rather than Reference Lines. In these cases, there is an option when ordering the MyPerioPath® or Alert 2™ to have the Reference Lines removed from the lab report. If the option for removal is selected, the systemic antibiotic option is still based off of the Reference Lines, and an antibiotic selection will appear only when levels exceed the threshold.
Just as with any medical lab report which shows the reference range for the particular test result, the Reference Lines serve as a reference range for clinical decision-making. Bacteria reported above the Reference Lines might be viewed as out of range, providing a cause for treatment if the patient is in a clinical state. If the patient is without clinical signs of disease and above the reference line, this might provide a cause for a proactive intervention. Bacteria detected at levels below the Reference Lines may be considered as in range, if the patient is absent of clinical signs, no therapy would be warranted as a baseline potentially established. However, if below the Reference Lines levels of bacteria with active clinical signs of disease, you know you must treat the patient to stimulate them to heal.

Diane’s holistic approach is enriched by her extensive knowledge of nutrition, seamlessly integrating it into her practice. Proudly rooted in the Midwest, she makes her home in Minnesota with her husband, where she continues to contribute meaningfully to the dental community, driven by a deep commitment to excellence and patient care.
- Update to MyPerioPath® Antibiotic Options: What You Need to Know - January 2, 2026
- Why Test? Rethinking Periodontal Disease Through a Medical Lens - August 1, 2025
- Practicing Dental Medicine: The Partnership with a Clinical Laboratory - December 13, 2024