
![]()
A patient presented for a new patient exam to our practice after many years of “routine” and “regular” cleanings elsewhere.
Although clinical and radiographic findings indicated chronic infection and the need for comprehensive non-surgical therapy including scaling and root planing, irrigation, and bacterial decontamination, the patient declined adjunctive care and requested to receive scaling alone.
Local anesthesia was administered, and scaling and root planning was performed.
This approach felt more familiar to the patient and, at first glance, reasonable.
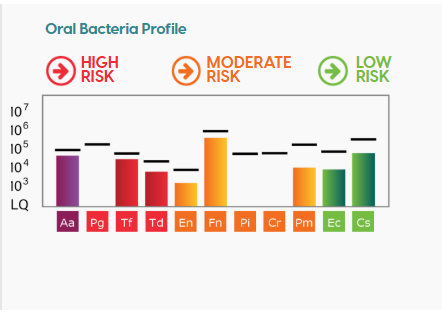
Below is the Patient’s baseline Alert 2 results:
 On the first maintenance, even after showing him these findings, the patient declined adjuncts again but allowed us to take a follow-up MyPerioPath (MPP). The patient had a mission to see if our recommendations were actually necessary.
On the first maintenance, even after showing him these findings, the patient declined adjuncts again but allowed us to take a follow-up MyPerioPath (MPP). The patient had a mission to see if our recommendations were actually necessary.
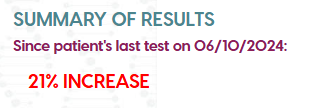
The follow-up MPP report revealed our expected outcome: a 21% increase in total bacterial load following scaling alone.
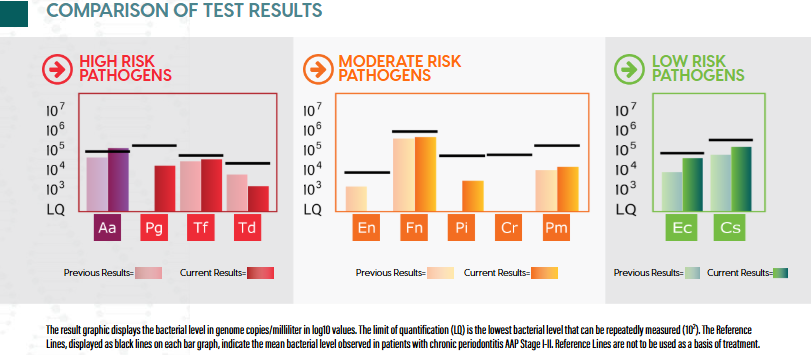
The mouth “felt cleaner” to the patient, but biologically, it was more active than before.
Armed with this evidence for their second maintenance, the patient agreed to proceed with the full recommended non-surgical protocol:
- Subgingival chlorhexidine irrigation (0.12%) delivered ultrasonically to every pocket.
- Gemini dual-wavelength laser decontamination (810 nm / 980 nm) applied at roughly 50 °C for 5–10 seconds per site.
A follow-up MPP demonstrated a sharp bacterial reduction: over 57% overall, with dramatic decreases in red and orange complex pathogens.
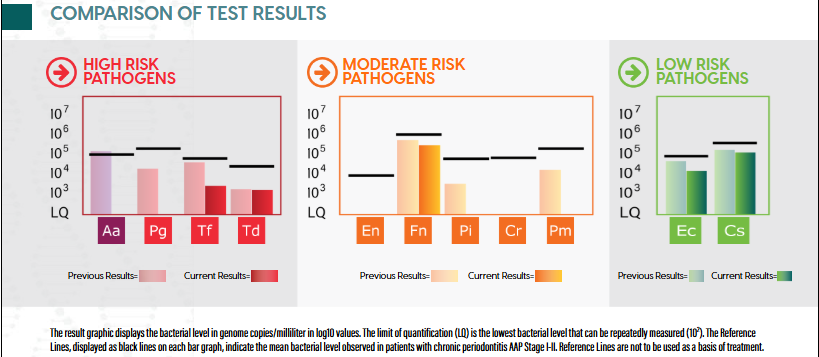
The only variable that changed was the introduction of adjunctive treatments.
So why did scaling alone fail? Mechanical scaling disrupts biofilm surfaces but rarely destroys the biofilm itself.
Without chemical or photothermal disruption, the extracellular polymeric substance (EPS) remains intact. Think of it like a gel-like fortress limiting diffusion of irrigants and protecting bacteria within 100 µm of depth.
Once the surface layer is removed, oxygen tension drops, and anaerobes rebound, often more aggressively.
Or in other words: The metal scaler has no disinfecting qualities, what is actually bactericidal is the Irrigation and Decontamination.
How Adjuncts Changed Biology
| Complex | Dominant Pathogens | Resistance Mechanisms | Adjunctive Mechanism of Action |
| Red Complex | P. gingivalis,
T. forsythia, T. denticola (1) |
Motile spirochetes invade collagen. (2) | Gemini 810 nm targets pigmented anaerobes; 980 nm penetrates water in EPS, reaching ~50 °C to denature proteins (3-4) |
| Orange Complex | F. nucleatum,
P. intermedia, C. rectus (1) |
Bridge organisms with catalase and efflux pumps that resist rinses. (5) | Laser heat deactivates catalase; CHX penetrates and lyses surviving cells. (3-4) |
| Early Colonizers | Capnocytophaga,
Eikenella, Actinomyces (6) |
Rapid recolonizers on residual surfaces. (7) | CHX substantivity maintains antimicrobial presence for hours, preventing early re-adhesion. (8) |
- The Gemini diode laser emits 810 nm and 980 nm wavelengths simultaneously.
- 810 nm is absorbed by pigmented bacterial enzymes, rupturing pathogenic cell walls.
- 980 nm is absorbed by water, producing a gentle microthermal field (~50 °C) that softens the EPS and exposes hidden bacteria.
- Chlorhexidine complements the laser-assisted bacterial reduction biologically and temporally:
- Pre-laser-assisted bacterial reduction: it saturates the pocket, providing immediate antimicrobial contact.
- Post-laser-assisted bacterial reduction: it binds to newly denatured surfaces, sustaining activity for up to 12 hours.
This dual-target strategy eradicates both pigmented anaerobes and moisture-shielded colonies while sparing surrounding tissue.
The sequence — scale → irrigate → laser — converts a mechanical cleaning into a biofilm-level decontamination event.
Microbiologically, after adjunctive therapy, bacterial counts across red and orange complexes decreased dramatically.
Clinically, after adjunctive therapy, inflammation subsided, bleeding minimized, and tissue tone normalized.
Thanks to this non-surgical approach the ecosystem shifted from pathogenic dominance to a great start towards our goal of a more balanced symbiosis.
The case underscores a simple truth:
Some patients become self-advocates immediately, others require longer, but with good faith and some data, we can chaperone anyone towards better mouth-body health.
References:
- Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr. Microbial complexes in subgingival plaque. J Clin Periodontol. 1998
- Lux R, Miller JN, Park NH, Shi W. Motility and chemotaxis in tissue penetration of oral epithelial cell layers by Treponema denticola. Infect Immun. 2001
- Harris DM, Jacques SL, Darveau R. The black bug myth: selective photodestruction of pigmented pathogens. Lasers Surg Med. 2016
- Al-Hamdani SH, Al-Rawi NH, Al-Timimi DJ. The efficacy of diode laser (810-980 nm) as an adjunct to non-surgical treatment of periodontitis on Porphyromonas gingivalis: a randomized split-mouth study. Iraqi J Laser. 2025
- Zilm PS, Rogers AH. Co-adhesion and biofilm formation by Fusobacterium nucleatum in response to growth pH. Anaerobe. 2007
- Kolenbrander PE, Andersen RN, Blehert DS, Egland PG, Foster JS, Palmer RJ Jr. Communication among oral bacteria. Microbiol Mol Biol Rev. 2002
- Teles FR, Teles RP, Uzel NG, Song XQ, Torresyap G, Socransky SS, Haffajee AD. Early microbial succession in re-developing dental biofilms in periodontal health and disease. J Periodontal Res. 2011
- Suárez-Rodríguez B, Regueira-Iglesias A, Blanco-Pintos T, Sánchez-Barco A, Vila-Blanco N, Balsa-Castro C, Carreira J, Tomás I. Randomised-crossover clinical trial on the substantivity of a single application of a gel containing chlorhexidine and o-cymen-5-ol on the oral biofilm and saliva. BMC Oral Health. 2024


- When Data Changes Minds: How Chlorhexidine Irrigation and Non-Surgical Laser Therapy Transformed a Resistant Microbiome in a Reluctant Patient - June 26, 2026
- Revolutionizing Periodontal Disease Screening and Treatment with OFC and Alert 2™ Diagnostics - October 25, 2024
- Dr. Benavides: “Did We Overtreat: The Value of Proactive Intervention for the Periodontal Patient.” - August 23, 2024