
![]()
For a long time, bleeding gums were treated as a home care conversation.
Brush better.
Floss more consistently.
Let’s keep an eye on it… but what are we actually waiting for?
That’s how most of us were taught. And honestly, it’s exactly how I practiced early in my career too.
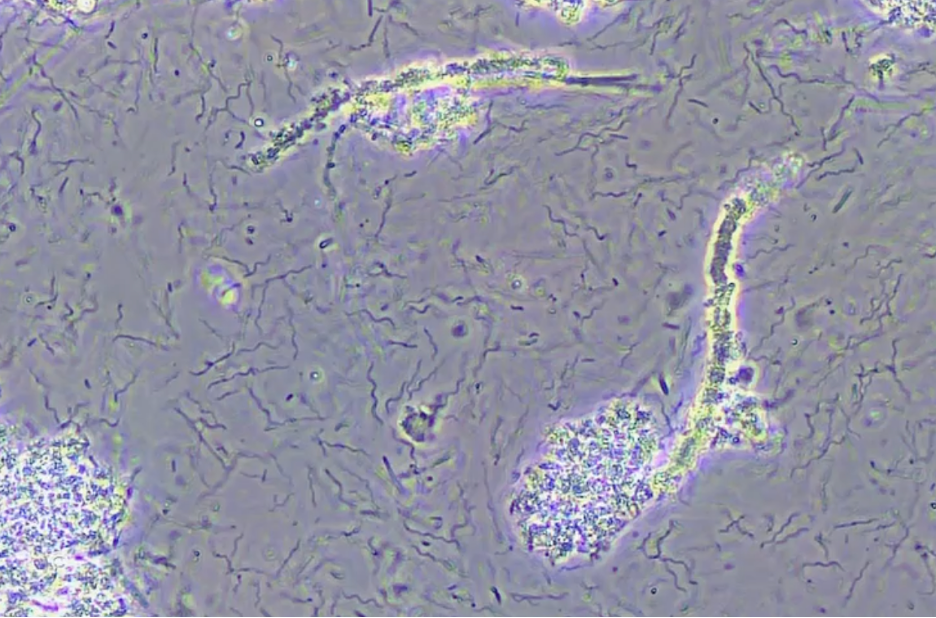
In 2008, when I began using salivary diagnostics alongside phase-contrast microscopy, something shifted for me. For the first time, I wasn’t making educated guesses. I could identify which microbes were present and better understand what was actually driving inflammation beneath the surface.
That clarity changed how I approached periodontal care.
A Patient Who Changed My Perspective
Sally was in her early 40s with excellent home care, a beautifully restored mouth, and two implants placed just 18 months earlier. She came to us because one implant already showed peri-implantitis with a vertical defect. The recommendation she’d been given was removal.
“Sometimes implants just fail.”
That explanation didn’t sit right with her. So, she looked for another perspective and found our practice, driving more than two hours because she wanted answers, not just a recommendation.
During her exam, I said, “Implants don’t usually fail without a reason. This looks like an infection. Let’s find out which bacteria may be involved.”
We completed a comprehensive evaluation and ran a MyPerioPath® test. The results helped explain why her implant was failing. The infection wasn’t isolated to the implant site; it reflected a broader microbial imbalance in the mouth.
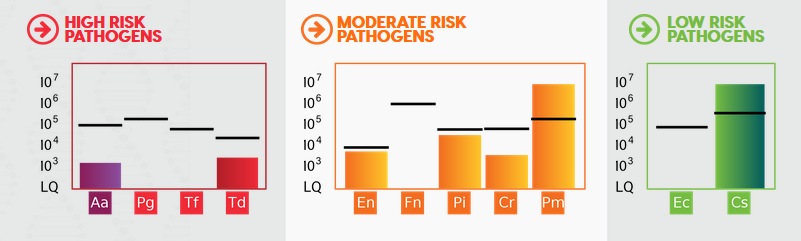
High-Risk (Aa)
Aggregatibacter actinomycetemcomitans (Aa)
-
- Highly aggressive pathogen linked to rapid tissue destruction
- Known for invading tissue and evading the immune system
- Frequently associated with bone loss around teeth and implants
High-Risk (Red Complex – Td)
Treponema denticola (Td)
-
- Motile spirochete strongly linked to peri-implantitis
- Disrupts tissue integrity and interferes with healing
- Often found in advanced periodontal and peri-implant infections
Moderate-Risk Pathogens (Orange Complex)
Prevotella intermedia (Pi)
-
- Inflammatory pathogen commonly elevated around failing implants
- Thrives in inflamed, low-oxygen environments
Campylobacter rectus (Cr)
-
- Associated with bone loss and peri-implant inflammation
- Frequently found alongside more aggressive pathogens
Transitional Bacteria (Cs)
Capnocytophaga species (Cs)
-
- While often a part of the normal flora, higher levels can reflect a shift away from a balanced biofilm
- Helps illustrate imbalance when outweighed by pathogenic species
- Helps illustrate imbalance when outweighed by pathogenic species
It wasn’t the presence of one bacteria that explained the problem, it was the combination and overall imbalance. Once we understood what was driving the inflammation, treatment became clearer and more targeted.
Treating the Whole Environment
Instead of focusing only on the implant area, we treated the entire oral environment.
-
- Full-mouth non-surgical periodontal therapy
- Targeted antimicrobial support
- Clear, realistic home care protocols
- Immune system support to help the body heal
We were honest with Sally. We couldn’t promise outcomes. But we could address the underlying drivers.
Within weeks, she said, “This is the best my mouth has ever felt.”
Eighteen months later, her radiographs told the rest of the story. Bone had regrown around the implant without grafting, with increased density and stability.
Why This Matters
Bleeding gums are often viewed as a surface-level issue. Yet many patients with excellent home care still show signs of inflammation. Traditional diagnostics show us what’s already happened. Salivary diagnostics and microscopy help us understand what’s driving change earlier.
And when we see things earlier, care gets simpler, not more complicated.
When patients can see and understand what’s happening, conversations shift. Treatment recommendations feel logical, not surprising.
Bleeding gums aren’t a failure.
They’re information.
This is the approach I teach, because I’ve seen this pattern repeat itself time and time again.
When we understand the microbial drivers and treat the whole environment – care becomes clearer, outcomes improve, and teams feel far more confident in the recommendations they’re making
Stay Awesome,
Tosha, RDH


She helps practices turn periodontal care into a clinical and financial asset by bringing clarity to hygiene—aligning diagnosis, communication, and treatment so patients understand the why, want the treatment, and hygiene becomes a reliable driver of practice growth.